Constipation is a common problem. It means either going to the toilet less often than usual to empty the bowels, or passing hard or painful stools (faeces). Constipation may be caused by not eating enough fibre, or not drinking enough fluids. It can also be a side-effect of certain medicines, or related to an underlying medical condition. In many cases, the cause is not clear. Laxatives are a group of medicines that can treat constipation. Ideally, laxatives should only be used for short periods of time until symptoms ease. At Colorectal Unit, we provide the best Constipation treatment in Mumbai

Constipation Treatment in Mumbai

What can I do to ease and to prevent constipation?
These measures are often grouped together and called lifestyle advice.
Eat foods that contain plenty of fibre
Fibre (roughage) is the part of plant food that is not digested. Fibre adds bulk and some softness to the stools. Increasing the fibre in your diet may take a few days or even a few weeks to work. You may find that if you eat more fibre, you may have some bloating and wind at first. As your gut becomes used to extra fibre, the bloating or wind tends to settle. So if you are not used to a high-fibre diet, it is best to increase the amount of fibre gradually. Aim for 30 g of fibre per day. Remember to drink plenty when you increase the fibre in your diet. Rarely, the guts can develop a blockage if too much fibre is eaten without enough fluid.
Have plenty to drink
Aim to drink at least two litres (about 8-10 cups) of fluid per day. You will pass much of the fluid as urine but some is passed out in the gut and softens the stools. Most sorts of drink will do, other than alcoholic drinks, which can lead to a lack of fluid in the body (dehydration). As a start, try just drinking a glass of water 3-4 times a day in addition to what you normally drink.
Sorbitol
Sorbitol is a naturally occurring sugar. It is not digested very well and draws water into the gut, which has an effect of softening the stools. So, you may wish to include some foods that contain sorbitol in your diet. Fruits (and their juices) that have a high sorbitol content include apples, apricots, gooseberries, grapes (and raisins), peaches, pears, plums, prunes, raspberries and strawberries. The concentration of sorbitol is about 5-10 times higher in dried fruit. Dried or semi-dried fruits make good snacks and are easily packed for transport – for example, in a packed lunch.
Other dietary measures
There is some evidence that prunes are as effective as one of the most used laxatives. About six prunes twice a day was found to be effective in one small study.
Exercise regularly, if possible
Keeping your body active helps to keep your gut moving. It is well known that disabled people, and bed-bound people (even if just temporarily whilst admitted to hospital) are more likely to become constipated.
Toileting routines
Do not ignore the feeling of needing the toilet. Some people suppress this feeling if they are busy. It may result in a backlog of stools which is difficult to pass later. When you go to the toilet, it should be unhurried, with enough time to ensure that you can empty your bowel.
When mobility is limited – for example, in people who are frail or who have dementia – it is important for carers to see that they have sufficient help to get to the toilet at the time they need to go; also, that they have a regular, unhurried toilet routine, with privacy. As a rule, it is best to try going to the toilet first thing in the morning or about 30 minutes after a meal. This is because the movement (propulsion) of stools through the lower bowel is greatest in the mornings and after meals (due to an effect called the gastrocolic reflex).
Positioning on the toilet is also important, especially for elderly people with constipation. Western-style toilets actually make things more difficult – squatting is probably the best position in which to pass stools. Putting a small footstool under your feet is a simple way to change your toilet position to aid the passage of stools. Relax, lean forward and rest your elbows on your thighs. You should not strain and hold your breath to pass stools.
Laxatives
Laxatives are the medicines most commonly used for constipation. Treatment with a laxative is needed only if the lifestyle measures above do not work well. It is still worth persisting with these methods, even if you end up needing to use laxatives.
For short-term uncomplicated constipation, you may even choose to treat yourself (without visiting the GP) by buying laxatives in the pharmacy or supermarket. In short-term constipation, laxatives can be stopped once the stools (faeces) become soft and easier to pass. You should probably visit your GP if you are struggling to manage short-term constipation yourself, or if you have longer-term (chronic, or persistent) constipation.
Chronic constipation can be more difficult to treat. Laxatives are usually needed for longer periods (sometimes even indefinitely) and they should not be stopped abruptly.
There are four main groups of laxatives that work in different ways. You can read about laxatives, the different types and when they are used, in the The laxative recommended by your doctor or pharmacist will depend on factors such as your own preference, the symptoms of constipation that you have, possible unwanted effects, your other medical conditions, and cost. You should use a laxative only for a short time, when necessary, to get over a bout of constipation. Once constipation eases, you should normally stop the laxative.
Other Constipation Treatment
Constipation is usually helped by the above measures and treatments. Mostly, laxatives are taken by mouth (orally). In some cases, it is preferable also to treat constipation by giving medication via the back passage (anus).
Suppositories are pellet-shaped laxatives that are inserted into the the lowest part of the colon (the rectum), via the anus. Glycerol suppositories act as a stimulant within the rectum, encouraging the passing of stools. Sometimes, an enema is needed in severe constipation. An enema is a liquid that is inserted into the rectum and lower colon, via the anus. Enemas can be used to clear out the rectum in severe constipation.
Newer medicines are occasionally used in people with chronic constipation in whom standard laxatives have not been effective. Prucalopride is a medicine which stimulates gut movement. and lubiprostone and linaclotide also affect fluid levels in the guts, helping to soften the stool.
Can there be any complications from constipation?
Short-term constipation or intermittent bouts of constipation are unlikely to cause any long-term problems. Sometimes a split or tear in the anal skin (an anal fissure) can occur with the passage of particularly big or hard stools (faeces). This is very painful and there may be a small amount of fresh red blood on tissues
Long-term or persisting (chronic) constipation and long-term use of laxatives can result in your bowel becoming sluggish and ‘lazy’. This means that the bowel doesn’t work very well on its own, without medication. Constipation then becomes a vicious cycle and even more chronic. Try to avoid getting into this situation in the first place by using laxatives for short periods of time only. Consult your GP for advice if you are needing them regularly. Some people with persistent and severe constipation do require regular laxatives.
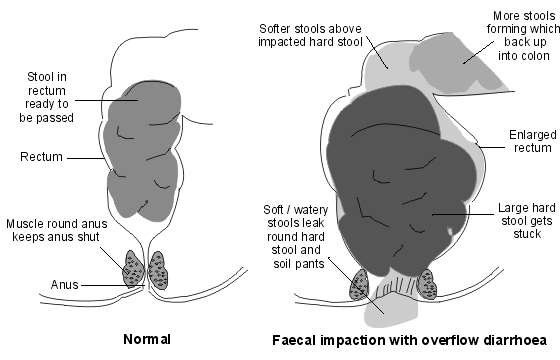
Severe chronic constipation can sometimes result in faecal impaction. In this condition, a large mass of hard faeces blocks the rectum. The mass is too big to pass and the rectum is stretched and enlarged, so the muscles within it don’t work so well and are unable to push the faeces out. Sometimes people with this problem think that they have diarrhoea. This is because liquid faeces, from above the blockage, leak around the hard lump of faeces and out of the anus. This is known as overflow diarrhoea. In this situation, you may also have faecal incontinence – that is, you have no control over this liquid faeces leaking out. Faecal impaction with overflow diarrhoea is likely if you have been getting progressively more constipated, and then have liquid faeces, possibly explosive, and without much control. If a doctor or nurse examines the anus, the hard faeces can often be felt, confirming the diagnosis. The diagram below shows this process:
In order to treat impaction, higher doses of laxatives need to be used, and sometimes enemas or suppositories. Temporarily, symptoms of diarrhoea may worsen but it is important to keep up with treatment, to clear the blockage. After the large mass of faeces is cleared, laxatives are often needed for a while (or perhaps even long-term or intermittently) to prevent the problem recurring.
Constipation in pregnancy
Constipation is a very common symptom in pregnancy. About 4 in every 10 pregnant women develop constipation. First steps to help are lifestyle changes to diet, fluid intake and keeping mobile discussed above. If these do not work, treatments are broadly the same, but of course not all medicines are safe in pregnancy. Your pharmacist, GP or midwife will be able to advise on the safest and most effective options for you
Constipation is common. The word may mean different things to different people as bowel habits differ between people. If you are constipated it causes one or more of the following:
- Stools (faeces) become hard and difficult or painful to pass
- The time between toilet trips increases compared with your usual pattern. There is a large range of normal bowel habit. Some people normally go to the toilet to pass stools 2-3 times per day. For others, 2-3 times per week is normal. It is a change from your usual pattern that may mean that you are constipated. In general passing a soft stool at least three times a week is considered normal.
- Sometimes, crampy pains occur in the lower part of your tummy (abdomen) You may also feel bloated and feel sick if you have severe constipation.
- It does not feel as though you have emptied your bowel or ‘finished’ after you have been to the toilet to pass a stool.
Chronic constipation means the problem has been present for at least 12 weeks out of the past 6 months.
What are the causes of constipation?
Some causes are known to lead to constipation, including the following:
- Not eating enough fibre (roughage) can lead to constipation. The average person in the UK eats about 12 g of fibre each day. However, 18 g per day is recommended by the British Nutrition Foundation. Fibre is the part of plant food that is not digested. It remains in your gut. It adds bulk to the stools (faeces) and helps your bowels to work well. Foods high in fibre include fruit, vegetables, cereals and wholemeal bread.
- Not drinking much may lead to constipation or make constipation worse. Stools are usually soft and easily passed if you eat enough fibre and drink enough fluid. However, some people need more fibre and/or fluid than others in order to avoid constipation.
- Some special slimming diets are low in fibre and may cause constipation. For example, diets very low in carbohydrates and some liquid diets.
- Some medicines can cause constipation as a side-effect. Examples are painkillers (particularly those with codeine, such as co-codamol, or very strong painkillers, such as morphine), some antacids, some antidepressants (including amitriptyline) and iron tablets; however, there are many others. See the list of possible side-effects on the leaflet that comes with any medicine that you may be taking. Tell a doctor if you suspect a medicine is making you constipated. A change of medication may be possible.
- Various medical conditions can cause constipation. For example:
- An underactive thyroid gland.
- Irritable bowel syndrome.
- Diverticular disease.
- Colon cancer.
- Being less mobile for various reasons, for example:
- Illness or injury.
- Disability
- Frailty or old age.
- Depression.
- Work patterns.
- Obesity
- Pregnancy About 1 in 5 pregnant women will become constipated. It is due to the hormonal changes of pregnancy that slow down the gut movements. In later pregnancy, it can simply be due to the baby taking up a lot of room in the tummy and the bowels being pushed to one side.
Unknown Cause (Idiopathic)
Some people have a good diet, drink a lot of fluid, do not have a disease and do not take any medication that can cause constipation; however, they still become constipated. Their bowels are said to be underactive. This is quite common and is sometimes called functional constipation or primary constipation. Most cases occur in women. This condition tends to start in childhood or in early adulthood and persists throughout life.