
Bowel Obstruction
In a bowel obstruction (intestinal obstruction), a blockage prevents the contents of the intestines from passing normally through the digestive tract. The problem causing the blockage can be inside or outside the intestine. Inside the intestine, a tumor or swelling can fill and block the inside passageway of the intestine. Outside the intestine, it is possible for an adjacent organ or area of tissue to pinch, compress or twist a segment of bowel.
A bowel obstruction can occur in the small bowel (small intestine) or large bowel (large intestine or colon). Also, a bowel obstruction can be total or partial, depending on whether any intestinal contents can pass through the obstructed area.
In the small intestine, the most common causes of bowel obstruction are:
Adhesions
Adhesions are areas of tough, fibrous connective tissue that are a type of scar. Adhesions develop on the outside of injured intestine or pelvic organs as they heal after surgery or infection. Gynecological surgeries and surgery involving the appendix or colon are particularly likely to result in adhesions. Adhesions do not always cause symptoms when they first form. Because of the motion of the intestine, it is common for these collections of scar tissue to be stretched into string-like or band-like tethers over time. An area of adhesions can cause obstruction of the small bowel if the adhesions are pulled into the shape of a constricting band, pinching a portion of the small intestine closed from the outside. Adhesions also can bind to neighboring loops of intestine, and later tighten, pulling the intestine into an abnormal configuration that limits the flow of intestinal contents. Adhesions are the most common cause of small-bowel obstruction in the United States, accounting for 50% to 70% of all cases.

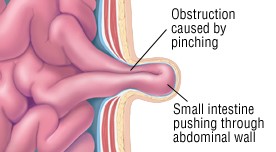
Hernia
If there is a structural weakness in the muscles and fibers that are part of the wall of the abdomen, a portion of the small intestine may protrude through this weakened area, and appear as a lump under the skin. This protruding segment of intestine is called a hernia. The section of small intestine that becomes a hernia can become obstructed if it is trapped or tightly pinched at the point where it pokes through the abdominal wall. In extreme cases, the pinched intestine also may “strangulate,” meaning the blood supply is cut off. Hernias are the second most common cause of small-bowel obstruction in the United States, accounting for about 25% of all cases. Typically, hernias appear as lumps near the navel (umbilical hernia), between the navel and breastbone (ventral hernia), at the site of a healed surgical incision (incisional hernia), near the groin (inguinal hernia), or at the front of the upper thigh (femoral hernia).
Tumors
Cancerous tumors can cause small-bowel obstruction either by pressing on the outside of the bowel and pinching it closed, or by growing within the wall of the intestine and slowly blocking its inner passageway. Cancers account for a small percentage of all small-bowel obstructions. In most cases, the tumor does not begin in the small intestine itself. More often, it is a cancer that has spread (metastasized) to the small bowel from another site in the colon, female reproductive tract, breast, lung or skin.
In the large intestine, the most common causes of bowel obstruction are:
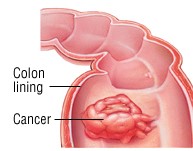
Colorectal Cancer
About half of all large-bowel obstructions are caused by colorectal cancer. Undiagnosed colon or rectal cancer may cause a gradual narrowing of the large intestine’s inner passageway. Usually patients experience intermittent constipation for a while before the bowel finally becomes obstructed.
Volvulus
Volvulus is an abnormal twisting of a segment of bowel around itself. This twisting motion typically produces a closed loop of bowel with a pinched base, leading to intestinal obstruction. In Western countries, volvulus is most common among people over age 65, and these patients often have a history of chronic (long-lasting) constipation.
Diverticular Disease
In the large bowel, diverticula are small, balloon-shaped pouches that protrude from the wall of the intestine. If diverticula become infected this is called diverticulitis. During healing from infection, scars may form in the wall of the colon as it. A scar that encircles the colon is called a colon stricture. As a stricture ages and tightens, it can narrow the intestine gradually, eventually causing a blocked colon.
Symptoms
Symptoms of small-bowel obstruction can include:
- Cramping abdominal pain, generally coming in intense waves that strike at intervals of five to 15 minutes and sometimes center either on the navel or between the navel and rib cage (Pain that becomes constant may be a symptom of bowel strangulation)
- Nausea and vomiting
- No gas passing through the rectum
- A bloated abdomen, sometimes with abdominal tenderness
- Rapid pulse and rapid breathing during episodes of cramps
Symptoms of large-bowel obstruction can include:
- A bloated abdomen
- Abdominal pain, which can be either vague and mild, or sharp and severe, depending on the cause of the obstruction
- Constipation at the time of obstruction, and possibly intermittent bouts of constipation for several months beforehand
- If a colon tumor is the cause of the problem, a history of rectal bleeding (such as streaks of blood on the stool)
- Diarrhea resulting from liquid stool leaking around a partial obstruction
Diagnosis
To diagnose a bowel obstruction, your doctor will need to feel and listen to your abdomen and feel inside your rectum. A blockage in the intestine is confirmed by X-rays of your abdomen, which show gas and liquid bowel contents above the area of the blockage, but no gas below the blockage. Blood tests must be done to check for dehydration or loss of electrolytes (such as sodium and potassium) if your symptoms have included vomiting.
If your doctor suspects you have a large-bowel obstruction, he or she may use a colonoscope, a tube that is inserted through the rectum to view the lower intestine. If the obstruction is caused by a volvulus, the passing of this instrument into the bowel not only confirms the diagnosis, but also untwists the intestine and relieves the obstruction.
It may not be possible to know the cause of a bowel obstruction unless surgery is done. Surgery permits a doctor to look at your intestine and at scar tissue if you have adhesions.
Expected Duration
Symptoms of small bowel obstruction and large bowel volvulus usually become severe over a period of hours. However, large-bowel obstruction caused by colorectal cancer or diverticular disease may worsen more slowly. Some patients have mild symptoms for several weeks or months before seeing a doctor. Once the diagnosis is made, a hospital stay is required and may last for several days. With successful treatment, the obstruction is relieved.
Prevention
You may be able to reduce your risk of some forms of bowel obstruction by modifying your diet and lifestyle. For example
- To help prevent colorectal cancer, eat a balanced diet low in fat with plenty of vegetables and fruits, don’t smoke, and see your doctor for colorectal cancer screening once a year after age 50.
- To help prevent hernias, avoid heavy lifting, which increases pressure inside the abdomen and may force a section of intestine to protrude through a vulnerable area of your abdominal wall. If you develop an abnormal lump under the skin of your abdomen, especially near your groin or near a surgical scar, contact your doctor.
- There is no proven way to prevent obstruction caused by diverticular disease, but some doctors believe that people with diverticular disease should follow a high-fiber diet and avoid foods that may become lodged in the diverticula, such as seeds and popcorn.
Treatment
If you have a bowel obstruction, you will be treated in a hospital. A flexible, lubricated nasogastric tube (NG tube) can be inserted through your nose into your stomach to help remove excess gas from your stomach and intestines. You will be given fluids intravenously (through a vein) because you will not be allowed to eat or drink.
Partial small-bowel obstruction often improves within a few days, and the NG tube can be removed if one was used. At that point, you will be given sips of fluid. If you tolerate this, you will be given a full liquid diet for a day or more followed by solid foods that are easy to digest. A complete bowel obstruction often requires surgery to correct or remove the cause of the obstruction (tumor, adhesions, stricture), repair the hernia, or fix the segment of intestine at risk of repeated volvulus. During this surgery, a segment of damaged or strangulated intestine also may be removed.
It is sometimes most practical for your doctor and you to take a “wait and see” approach if you recover from one or two episodes of bowel obstruction without surgery. You may eventually require surgery to correct the cause of the blockage or to prevent future episodes, but not everyone needs surgery.